
Introduction
This edition of the ISODP Journal Watch highlights how policy, metrics, and technology are converging to reshape organ donation and transplantation worldwide, themes that sit squarely within ISODP’s mission to promote ethical, effective practices across diverse systems. Two complementary papers revisit presumed consent and soft opt-out models, reminding readers that law reform alone does not guarantee higher donation rates and that family roles, trust, and implementation detail remain critical determinants of success. At the system level, new work from the Global Observatory and European collaborators offers more nuanced ways to understand and benchmark performance, from age-stratified donation rates that expose untapped potential in older decedents to a validated, multi-domain indicator set for donation and transplant programme scorecards. Alongside these policy and measurement advances, clinical innovation continues to push boundaries: pioneering pediatric DCD heart transplantation using hypothermic oxygenated perfusion suggests a path to greater equity for children with end-stage heart failure who have historically had limited access to donor hearts. Taken together, these articles underscore that, in line with ISODP’s strategic priorities, closing the gap between need and transplantation will require coordinated progress in legislation, public engagement, system design, and technology rather than reliance on any single lever.
Dr. Helen Opdam
(Intensive Care Specialist)
helen.opdam@austin.org.au
Dr. David Thomson
(Critical Care and Transplant Surgeon)
thomson.david@gmail.com

HOPE for children: successful pediatric DCD heart transplantation using hypothermic oxygenated perfusion
Chilvers, Nicholas J.S. et al.
The Journal of Heart and Lung Transplantation, March 2026
Corresponding author: Louise Kenny - louise.kenny4@nhs.net
This article reports the first clinical experience of pediatric donation after circulatory death (DCD) heart transplantation using hypothermic oxygenated perfusion (HOPE), together with supporting preclinical work in small porcine models. The study was developed in response to the major shortage of pediatric donor hearts, especially for infants and small children, and to the fact that existing DCD heart technologies have been difficult to apply in smaller donors.
The authors combined animal feasibility work with a six-patient clinical series from the UK and Belgium, including 3 DCD and 3 DBD pediatric donor hearts preserved using HOPE. They developed modified cannulation techniques, including arch vessel cuff creation and aortic arch augmentation, to allow preservation of hearts from very small donors, including donors as small as 9 kg in the clinical series.
The findings are striking. In the DCD cohort, median functional warm ischemic time was 19 minutes, no severe primary graft dysfunction occurred, and survival at follow-up was 100%, with normal systolic function reported on echocardiography. Across the whole cohort, all recipients were alive at a median follow-up of 287.5 days, and the authors argue that these donor hearts would likely not have been transplanted without HOPE.
This paper is important because it suggests a practical way to extend heart donation to younger pediatric DCD donors and potentially improve equity for children waiting for transplant. Although the study is small and technically demanding, it offers encouraging early evidence that HOPE may safely expand the pediatric heart donor pool where legislative, ethical, and surgical capability permit its use.
Summary prepared by Dr. Helen Opdam
Together, the next three articles turn the spotlight from individual cases to the performance of whole donation and transplant systems and to how they can be measured more intelligently over time. The Global Observatory report provides the broad global picture of activity and unmet need, while age-stratified analyses reveal where apparently similar systems differ markedly once donor age is taken into account, and where the greatest unrealized potential lies. Building on this, a new consensus-based indicator set offers a practical scorecard for national programmes, integrating traditional activity measures with equity, prevention and long-term outcomes to support more meaningful benchmarking and quality improvement across countries.
Organ Donation and Transplantation Worldwide: The Global Observatory on Donation and Transplantation 2024 Report
Martin, Friederike et al.
Transplantation, March 2026
Corresponding author: Friederike Martin - friederike.martin@charite.de
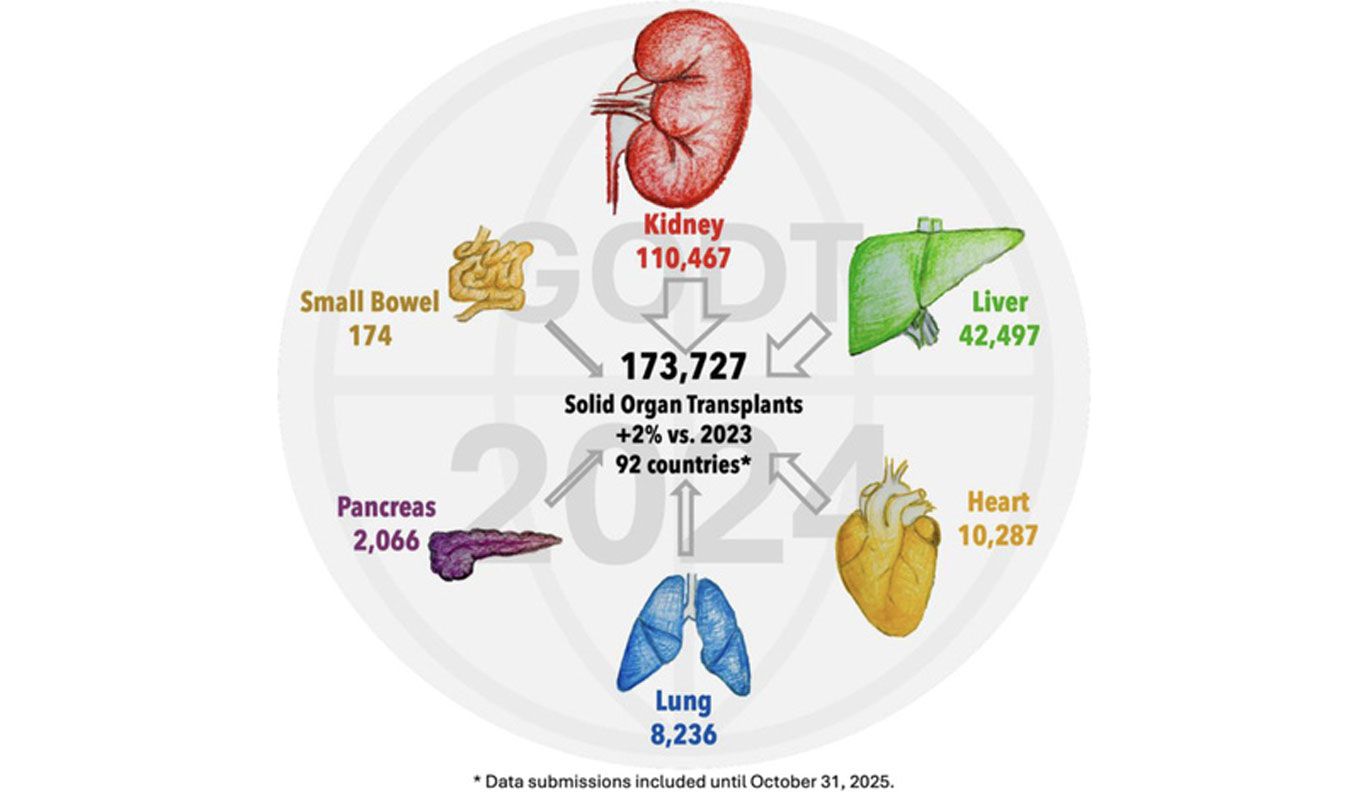
This annual report presents a global overview of solid organ donation, transplantation, and waitlisting activity, using data submitted to the Global Observatory on Donation and Transplantation (GODT) from 92 countries for 2024. It provides a broad picture of worldwide transplant activity, with attention to donor type, regional variation, and persistent inequities in access.
The report found that 173,727 solid organ transplants were performed worldwide in 2024, the highest number yet reported to the GODT, representing a 2% increase from 2023. This growth was driven largely by deceased donation, particularly donation after circulatory determination of death (DCD), which accounted for 28% of all deceased donors and increased by 17% compared with the previous year.
Despite this progress, the report also highlights the continuing imbalance between need and supply. A total of 668,160 patients were reported as waitlisted for transplant during 2024, and 31,853 died while waiting, underscoring how far global systems still are from meeting demand. The burden was not shared equally, with most transplant activity concentrated in the Americas and Europe, while access remained markedly lower in many other regions.
This is an important systems-level paper for the donation community because it shows both what is possible and where the major gaps remain. It reinforces the value of DCD program development, donor utilization, living donation protections, and stronger national infrastructure, while also reminding readers that transparency and reliable international benchmarking are essential if global donation and transplantation systems are to improve.
Summary prepared by Dr. Helen Opdam


Organ Donation and Transplantation Worldwide: The Global Observatory on Donation and Transplantation 2024 Report
Martin, Friederike et al.
Transplantation, March 2026
Corresponding author: Friederike Martin - friederike.martin@charite.de
This annual report presents a global overview of solid organ donation, transplantation, and waitlisting activity, using data submitted to the Global Observatory on Donation and Transplantation (GODT) from 92 countries for 2024. It provides a broad picture of worldwide transplant activity, with attention to donor type, regional variation, and persistent inequities in access.
The report found that 173,727 solid organ transplants were performed worldwide in 2024, the highest number yet reported to the GODT, representing a 2% increase from 2023. This growth was driven largely by deceased donation, particularly donation after circulatory determination of death (DCD), which accounted for 28% of all deceased donors and increased by 17% compared with the previous year.
Despite this progress, the report also highlights the continuing imbalance between need and supply. A total of 668,160 patients were reported as waitlisted for transplant during 2024, and 31,853 died while waiting, underscoring how far global systems still are from meeting demand. The burden was not shared equally, with most transplant activity concentrated in the Americas and Europe, while access remained markedly lower in many other regions.
This is an important systems-level paper for the donation community because it shows both what is possible and where the major gaps remain. It reinforces the value of DCD program development, donor utilization, living donation protections, and stronger national infrastructure, while also reminding readers that transparency and reliable international benchmarking are essential if global donation and transplantation systems are to improve.
Summary prepared by Dr. Helen Opdam

Age-stratified data highlight worldwide variability in organ donation rates and the potential increase in organ donation
Gaddipati, Sirisha et al.
Transplantation, March 2026
Corresponding author: David S. Goldberg - dsgoldberg@miami.edu
This study challenges the routine use of donors per million population as the main benchmark for international comparison of deceased organ donation, arguing that such metrics fail to account for differences in the age distribution and associated numbers of deaths between countries. The authors instead propose age-stratified donation rates (donors per 1000 deaths within age bands) as a more meaningful way to assess performance and identify growth potential.
Using World Health Organization mortality data and deceased donor data from 17 countries across Europe, North America, South America, and Oceania they calculated donation rates in seven age groups from 0–19 up to 70 years and older over the period 2013–2019. They also modelled how many additional donors each country might have achieved if its age-specific donation rates matched those of the best-performing country in each age band.
Overall donation rates varied about four-fold between countries, but age-stratified analysis revealed much larger differences within specific age groups, including a ten-fold gap in donation rates among people aged 70 years and older. The United States had relatively high donation rates among younger adults but much lower rates than Spain in older age groups, while countries such as Argentina, Germany, and Hungary showed substantial unrealised potential, especially among older decedents.
The authors conclude that age-stratified donation rates provide a more accurate and actionable measure of system performance than global per-million-population metrics. They suggest that focusing on older age groups, where deaths are most frequent but donation rates are often low, offers the greatest opportunity to expand deceased donation, provided that systems address organisational, clinical, and cultural barriers to using older donors.
Summary prepared by: Dr. Helen Opdam

Performance indicators for organ donation and transplantation programmes in Europe: modified Delphi consensus study
Streit, Simon et al.
BJS (British Journal of Surgery), 2026
Corresponding author: George Wharton - g.a.wharton@lse.ac.uk
This study addresses a key gap in donation and transplant system governance: the lack of an agreed, comprehensive set of indicators to assess the performance of national organ donation and transplantation programmes, beyond centre-level clinical metrics. The authors set out to develop a standardised “scorecard” of indicators suitable for comparing and monitoring national donation and transplant systems.
They used a three-step process: a targeted review of regulatory documents, national transplant organisation reports and existing databases to identify candidate indicators; expert mapping of these indicators to an established transplant system framework; and a two-round modified Delphi process with 30 international experts, including clinicians, policy researchers, system leaders and patient representatives. Across the Delphi rounds, 168 indicators were rated on importance, with consensus for inclusion defined as at least 80% of experts rating an indicator as “maybe include” or “include.”
Of the 168 indicators evaluated, 103 reached consensus and, after consolidating overlapping organ-specific measures, a final set of 84 indicators was produced. These were organised into seven domains: monitoring and reporting, prevention and need, waiting lists, consent, donation, transplantation, and follow-up, and included both familiar metrics (such as donation and transplant rates, waiting list size, graft survival and complication rates) and newer system-level measures addressing equity, patient-centredness, and structural capacity. Within this set, 25 indicators were classified as very high priority, including consent and family refusal rates, DBD and DCD rates per million population, numbers of pre-emptive kidney transplants, waiting time measures, and 1-, 5-and 10-year graft survival.
The authors argue that this validated indicator set can be used to construct national and cross-country “scorecards,” complementing qualitative system reviews and helping identify where reforms are most needed. Although implementation will require work on data availability, standardisation and equity-focused reporting, the framework offers policymakers and transplant leaders a practical tool to track progress, benchmark performance and align system goals around outcomes that matter to both professionals and patients.
Summary prepared by Dr. Helen Opdam
Opt-out legislation continues to attract political attention as a potential lever to increase deceased donation, but these final two papers underline that law change is neither a magic bullet nor a simple binary choice. Both argue that the impact of opt-out depends heavily on family roles, implementation details, infrastructure and public trust, rather than default rules alone.


Impact of opt-in versus opt-out organ donation legislation on donation rates: a systematic review
Abbasi, Mahmoud et al.
Journal of Perioperative Practice, 2026
Corresponding author: Katayoun Najafizadeh - katynajafi@yahoo.com
This systematic review examines whether moving from opt-in to opt-out consent systems reliably improves organ donation rates and what contextual factors modify any effect. The authors searched major databases and grey literature in October 2024, ultimately including 13 primary studies of legislative models and donation outcomes across multiple countries.
The included studies spanned cross-country panel analyses, within-country before-and-after evaluations and policy case studies. Some analyses reported higher deceased donation rates in countries with presumed consent, or increases after transition to opt-out laws, while others found no effect or even declines when legislative change was poorly implemented or met with public mistrust, as seen in Chile and Brazil.
The review highlights that family consent practices, registry design, broader donor policy, and health system capacity are critical modifiers. Presumed consent appeared most effective where families are still engaged, infrastructure and ICU capacity support donation, public campaigns accompany law change, and registry systems are clear; in contrast, without these elements, opt-out policies alone did little or were counterproductive.
Overall, the authors conclude that opt-out legislation can contribute to increased deceased donation but is not a universal or stand-alone solution. They recommend multifaceted strategies that combine legal frameworks with investment in donor identification, family approach, public education, and trust-building, tailored to each country’s cultural and legal context.
Summary prepared by Dr. Helen Opdam

Denmark Introduces a Soft Opt-out Organ Donation Law
Albertsen, Andreas
Transplantation, 2026
Correspondence: aba@ps.au.dk
This commentary describes Denmark’s 2025 transition from an opt-in to a soft opt-out organ donation law and situates it within the wider European policy landscape. Under the reform, all residents over 18 who had not previously registered a decision are now entered in the donor register as having “full permission – not confirmed,” signalling willingness but still requiring family approval for organ retrieval.
The legal options for individuals remain: full permission, limited permission, “don’t know” (family decides) or explicit refusal, with registered permission providing a sufficient legal basis for donation. The paper contrasts Denmark’s model with the Netherlands, where “not opposed” status itself authorises retrieval (subject to family veto), and England, where absence of a recorded decision is treated as consent but families can still block donation, arguing that all three systems reinterpret non-response as passive consent but differ in legal framing and the formal strength of the default.
The author notes that Denmark reached record deceased donor numbers in 2024 (125 donors), driven partly by increased use of DCD, before the law came into force, and that annual donor numbers have fluctuated over the past decade. Early effects of the law are seen primarily in registration behaviour: by August 2025, 36% of Danes aged 15 and older were in the register (up from 30% at the start of the year), with more people recording both consent and refusal, suggesting heightened engagement rather than a simple shift towards donation.
The legislation sits within a broader national action plan, “United in giving life back,” which also includes professional training, electronic reminders, promotion of living donation and public campaigns, with formal evaluation planned for 2029 and a commitment to consider further measures if donation does not increase. The commentary concludes that, given the success of some opt-in systems and ongoing debate over the effectiveness of defaults, Denmark offers an important new reference point for assessing modest, soft opt-out reforms embedded in a wider strategy.
Summary prepared by Dr. Helen Opdam
Social
Contact
Address
International Society for Organ
Donation Professionals
c/o The Transplantation Society
740 Notre-Dame Ouest
Suite 1245
Montréal, QC, H3C 3X6
Canada