

Dear IPTA Members,
We extend our heartfelt gratitude for your enthusiastic participation in applying for IPTA Committees and Communities. We are pleased to announce that we have now almost finalized the composition of both, and the inaugural meetings of the majority of the new Committees are taking place. Full details of the new Committee members will become available in the coming months.
We are also excited to commence the first organ-specific Community meetings in May. These are open to all. Please contact Katie Tait (IPTA Section Manager) at katie.tait@tts.org if you are interested in joining a community.

Update
Dear IPTA Members,
IPTA Education Committee Unveils Exciting Developments and Initiatives for 2024
In a bid to elevate pediatric transplant education to new heights, the IPTA Education Committee has unveiled its latest endeavors and initiatives for the year 2024. With a steadfast commitment to spearheading educational leadership in pediatric transplantation across various levels of training and expertise, the Committee has been hard at work crafting comprehensive educational activities tailored to meet the diverse needs of its global membership base.
One of the Committee's flagship projects is the establishment of the SMARTER Initiative, a groundbreaking endeavor that is a veritable treasure trove of monthly educational materials, ranging from podcasts to journal club presentations. This initiative, centered on pediatric transplantation, has delved deep into the realms of cardiac and lung transplantation research, shedding light on the intricate nuances, recent breakthroughs, and potential future trajectories in pediatric solid organ transplantation.
Visit the SMARTER Initiative Page
Looking ahead, the Education Committee is gearing up for a Virtual Education Symposium, slated to unfold in late 2024, specifically tailored for Fellows and Allied Health & Nursing Professionals (AHNP). The symposium promises to be a platform brimming with insightful discussions, cutting-edge research presentations, and invaluable networking opportunities, with further details set to be disclosed in due course.

Meanwhile, the Committee continues to work on responses for its survey aimed at gauging knowledge gaps and fostering innovation in education for IPTA Fellows. Comprising of 29 meticulously crafted questions, this survey seeks to refine the delivery of educational content and craft robust curriculum to empower future pediatric transplant professionals. Available in both English and Spanish, the survey aims to accommodate the preferences of participants, underscoring the Committee's commitment to inclusivity and accessibility.
The Education Committees of both IPTA and TTS are collaborating on a webinar for the 2024 TTS Education Committee program, focusing on assessing healthcare transition readiness among pediatric organ transplant recipients. Organized by Rupesh Raina and Stephen Marks on behalf of the IPTA Education Committee, the webinar targets solid organ transplant fellows, surgeons, and nephrologists. Scheduled for June 2024, the webinar aims to evaluate transition tools' effectiveness and compare outcomes between participants in transition programs and those who are not. The session will feature speakers covering various aspects of healthcare transition, followed by a panel discussion. With a diverse panel and multidisciplinary approach, the webinar seeks to enhance understanding of transition challenges and strategies.
This initiative demonstrates IPTA's commitment to disseminating knowledge and fostering collaboration among healthcare professionals worldwide. Through educational activities like webinars, IPTA endeavors to address critical issues in pediatric transplantation and enhance patient care across different regions and healthcare settings.
As the IPTA Education Committee forges ahead with its visionary endeavors, the pediatric transplant community eagerly anticipates the transformative impact of these initiatives on the landscape of pediatric transplantation education.

Update
Applications for the 2024 Outreach Program are Open

Visit the Outreach Program Page
New! Global Pediatric Transplant Centres Map
The IPTA Advocacy Team, an integral part of the Outreach Committee, comprises pediatric hepatologists, nephrologists, and cardiologists specializing in the treatment of children undergoing transplantation procedures globally. Our primary objectives revolve around evaluating international policies concerning pediatric transplantation allocation, pinpointing areas of knowledge deficiency, fostering critical understanding, and enhancing transparency. Through these efforts, we endeavor to establish an ethical framework for the allocation of deceased organs to pediatric recipients. Our ultimate aspiration is to champion the adoption of this framework on a global scale, thereby refining pediatric organ allocation protocols.
This project's goals harmonize seamlessly with the overarching endeavors of the IPTA Outreach Committee. They are poised to offer invaluable guidance to pediatric programs engaged in transplantation initiatives or seeking to enhance existing practices. By promoting transparency and advocating for high standards, our mission is to facilitate the delivery of exceptional and safe pediatric transplantation services worldwide.
Among the initiatives spearheaded by the IPTA Advocacy Team is the development of an interactive map showcasing medical centers offering pediatric transplantation services across the globe. This dynamic map will undergo regular updates to reflect the evolving landscape of pediatric transplantation facilities. Its purpose is to provide both healthcare providers and patients with a comprehensive resource, aiding in informed decision-making and fostering accessibility to specialized care.
See the link below to view the map. Please let us know if you know of any centers that are not included here and we will add!
Outreach Fellowship Winners announced soon!


Join IPTA Today!
Spread the word! If you know someone who you feel should become an IPTA member, please share this link https://tts.org/ipta-members-area/ipta-join or ask them to email sections@tts.org
Let’s keep up this momentum and grow the Society to 1000+ members!



Newsletter Discussion Corner
Equitable Access to Transplant Infrastructure and Resources for Pediatric Transplant Recipients
Behind the life-saving promise of organ transplantation lies a stark reality: the availability of resources for pediatric transplant care significantly lags behind adult programs. This inequity not only impacts the quality-of-care delivery, but in some cases precludes the establishment of pediatric transplant services altogether. In response to this pressing issue, the IPTA will formulate a position statement to illuminate the multiple facets of this issue, with input from the membership. The goal will be to empower IPTA members to advocate more effectively for equitable access, to dismantle systemic barriers and promote fairness in resource allocation.
There are several significant disparities present within pediatric and adult transplant care. These inequities include differences in access to medical facilities (both proximity and pediatric specialization), transplant specialized nursing, allied health, medical and surgical services, and dedicated funding of research and innovation – especially those innovations that must be tailored to varying pediatric-sized recipients. Consider the following case scenarios:
Patient Profile 1:
A 12-year-old diagnosed with atypical hemolytic uremic syndrome (aHUS) leading to renal failure requiring a kidney transplant. He resides in a rural area, far from the single pediatric transplant centers in his country, which burdens the family with long distances to travel with high transportation costs and extended periods away from home.
Patient Profile 2:
A 9-year-old is diagnosed with acute liver failure (ALF) and is in need of an urgent liver transplant. Despite having a pediatric transplant center in their region, the facility is small with a general pediatric mandate, and aside from medical expertise lacks transplant-specialized personnel that is available in larger adult transplant centers. Smaller numbers of patients limit personnel numbers and specialized capacity building due to turnover. The result is delays in treatment, longer waiting times for transplant assessments, and potentially inferior outcomes for pediatric patients.
Considering these two scenarios:
What aspects are similar to resource struggles you experience in your own institution – and what others do you notice? What supports are available from the adult transplant programs and what resource differences do you perceived relative to those available for adults? What information would you need to advocate for better resources to care for your patients?
The disparities in resource availability between pediatric and adult transplant programs are multifaceted, involving socioeconomic and demographic factors. One primary challenge lies in funding allocation, where pediatric programs may receive less financial support compared to their adult counterparts. This financial shortfall translates into limited infrastructure, staffing, and research opportunities in pediatric transplant centers. Additionally, geographic disparities exacerbate existing healthcare inequities, as children in rural or underserved areas face major barriers in accessing specialized pediatric transplant care, leading to delayed interventions and inferior outcomes.
The Ethics Committee is developing a position statement to recognize the urgent need to address these disparities and advocates for equitable access to pediatric transplantation. Addressing age discrimination, geography, and other factors influencing health disparities ensures that all children, regardless of their circumstances, have equal access to life-saving transplantation services. To achieve this goal, the statement will propose specific advocacy recommendations aimed at dismantling systemic barriers and promoting fairness in resource allocation to children.

Case Report
Case Report: Re-Transplantation in a Girl with End-Stage Renal Disease Secondary to Focal Segmental Glomerulosclerosis and Failure of Her First Transplant due to Recurrence
According to the NAPCRTS registry, recurrence of the primary disease accounts for 7-8% of graft losses in pediatric kidney transplant (KTx) recipients1. In those with focal segmental glomerulosclerosis (FSGS), recurrence is diagnosed in up to 60%2, and risk of graft loss is significantly higher than in patients with other etiologies of glomerulonephritis (42 vs 6.9%)3.
Limited data suggest that KTx recipients with graft failure due to recurrence of FSGS who then get a second transplant have an increased risk of recurrence and graft failure compared to the first transplant4. However, a recent collaborative case-control study including 20 patients with FSGS and a second transplant, found that, despite 70% of recurrence, second transplants had better graft survival than first ones, likely because recurrence was less severe and closely monitored5.
In this report we show the outcome of a pediatric KTx recipient with FSGS who lost her graft because of recurrence of nephrotic syndrome and two years later received a second transplant with a living-related donor graft from her father.
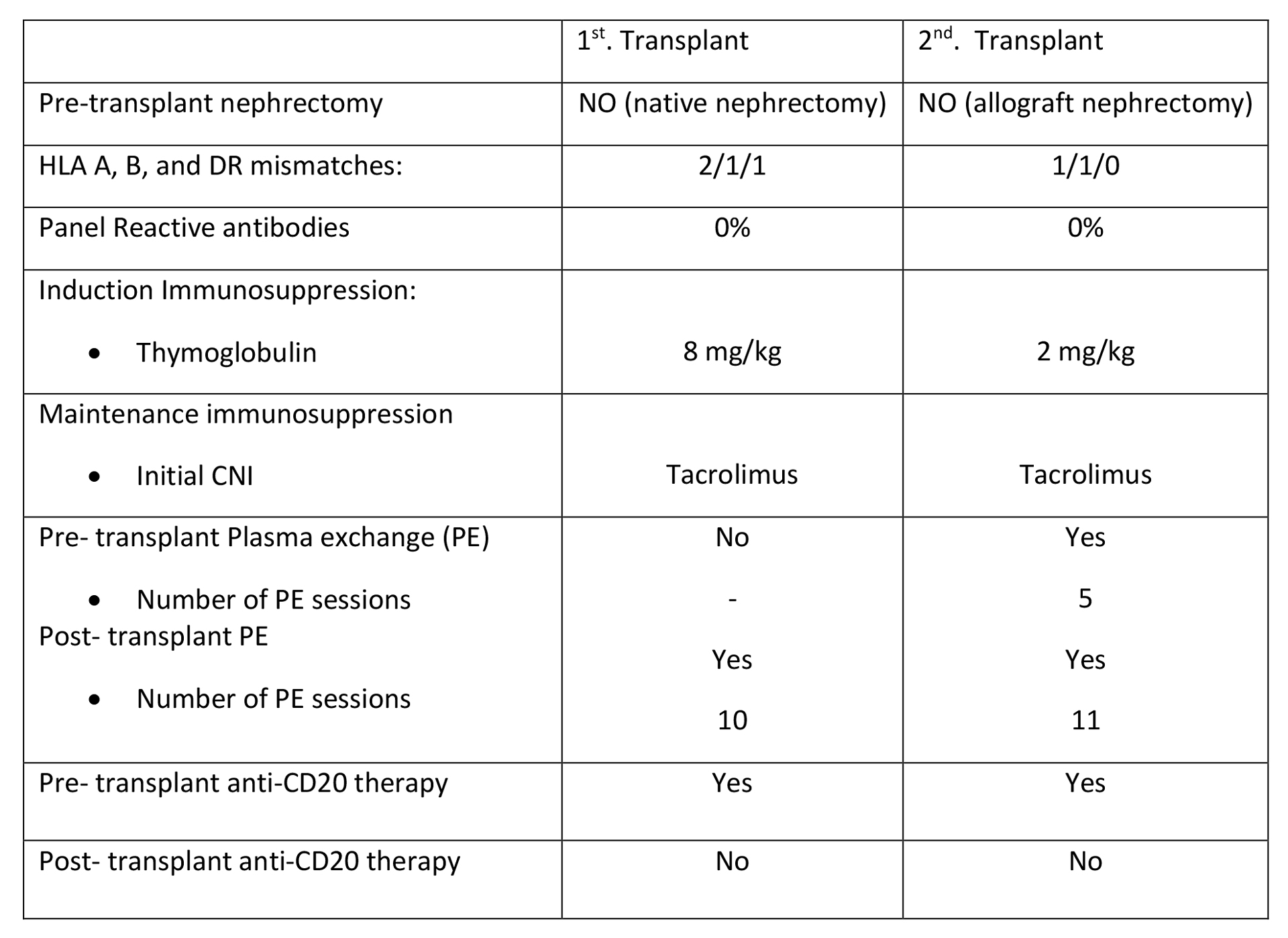
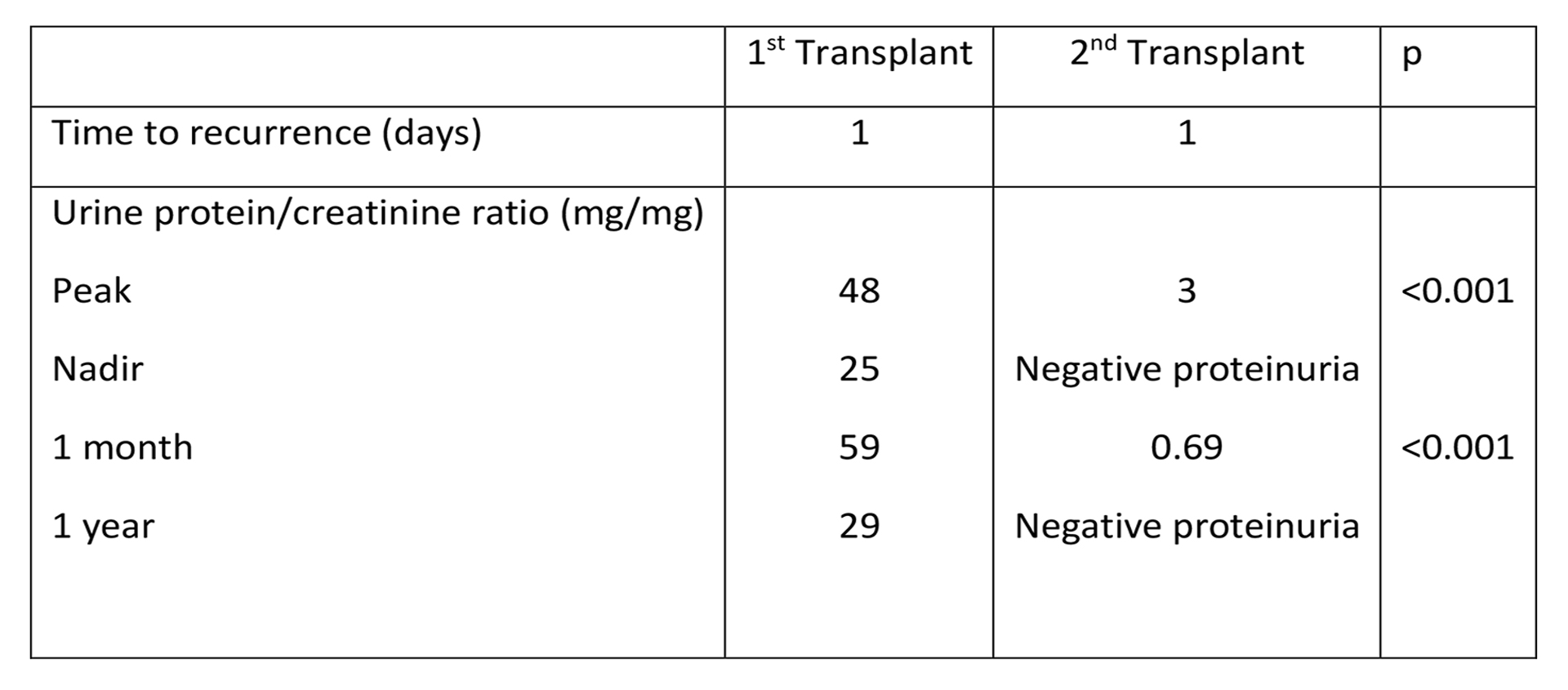
The patient was a 7-year-old Hispanic girl. Her weight was 18.2 kg (-0.99 SD) and height 107 cm (-1.99 SD). At three months of age, she developed nephrotic syndrome that progressed to chronic renal failure (CRF). Histology of her kidney biopsy revealed FSGS. Pre-transplant genetic testing (Next Generation Sequencing) did not identify any monogenic etiology. When she was 3.4 years old, with a body weight of 12.6 kg (-1.14 SD) and a height of 87 cm (-2.68 SD), she received a preemptive KTx from a deceased donor. Post-transplant, she had an immediate and severe (random urine protein/creatinine ratio of ≥2 mg/mg, serum albumin <2.5g/dl) recurrence of the nephrotic syndrome. Although diuresis was preserved, nephrotic-range proteinuria and low glomerular filtration rate persisted. Biopsy findings at 18 days and 10-month post-KTx were acute tubular necrosis, C4d negativity by immunofluorescence (i0 t0 v0 g0 cpt0 mm0 iT0 iFIAT- ci0-1 ct0 cv1 ah0 aah0 cg0)*, and minimal morphological changes (mesangial expansion, fibrosis, and minimal-to-mild interstitial inflammation (i0 t0 v0 g0 cpt0 mm0 iT0 iFIAT- ci0-1 ct1 cv0 ah0 aah0 cg0)*, without evidence of rejection. In October 2022, 18 months after KTx , she lost her graft because of recurrence and was started on peritoneal dialysis. In May 2023, she received her second graft. On the first day after KTx, serum creatinine was 0.28 mg/dl, eGFR 135 ml/min/1.73, random urine protein/creatinine ratio ≥2 mg/mg, and serum albumin <2.5g/dl. Proteinuria progressively decreased and 9 months post-KTx it was within the physiological range (urine protein/creatinine < 0.5 mg/mg) and continued to be so at the time of this report. She had no donor-specific antibodies (Luminex technique). Her nadir protein/creatinine ratio was lower after the second transplant compared to the first; peak values were higher after the first transplant.
The clinical course of this patient is consistent with the findings of Maniar et al5: in patients with FSGS second transplants are associated with better graft survival compared to the first transplant despite high recurrence rates, likely because recurrence after the second transplant is less severe compared to that after the first. However, one question remains: Will the outcome be the same if graft loss were due to recurrence together with rejection, and not recurrence alone? A prospective study in these children is needed.
(* - Electron Microscopy was not available.)
PATIENT DEMOGRAPHICS, IMMUNOSUPPRESSION AND PLASMAPHERESIS
POST-TRANSPLANT RECURRENCE OF FSGS AND PROTEINURIA
References
- Chua A, Cramer C, Moudgil A, et al. Kidney transplant practice patterns and outcome benchmarks over 30 years: the 2018 report of the NAPRTCS. Pediatr Transplant. 2019;23: e13597.
- Cochat P, Frague S, Mestrallet G, et al. Disease recurrence in pediatric renal transplantation. Pediatr Nephrol. 2009; 24:2097-2108.
- Koh LJ, Martz K, Blydt-Hansen TD; NAPRTCS Registry Investigators. Risk factors associated with allograft failure in pediatric kidney transplant recipients with focal segmental glomerulosclerosis. Pediatr Transplant. 2019 Aug;23(5): e13469.
- Jungraithmayr TC, Hofer K, Cochat P, Chernin G, Cortina G, Fargue S, Grimm P, Knueppel T, Kowarsch A, Neuhaus T, Pagel P, Pfeiffer KP, Schäfer F, Schönermarck U, Seeman T, Toenshoff B, Weber S, Winn MP, Zschocke J, Zimmerhackl LB. Screening for NPHS2 mutations may help predict FSGS recurrence after transplantation. J Am Soc Nephrol. 2011 Mar;22(3):579-85.
- Maniar A, Hooper DK, Sethna CB, Singer P, Traum A, Benoit E, Kotzen E, Verghese P, Garro R, Kamel M, Ranch D, Shih W, Jain NG, Al-Akash S. Re-transplantation in pediatric patients with failure of primary transplant due to recurrent focal segmental glomerulosclerosis: A pediatric nephrology research consortium study. Pediatr Transplant. 2021 Nov;25(7): e 14085.
Past Issues
IPTA Newsletters
- IPTA Newsletter - June 2026
- IPTA Newsletter - February 2026
- IPTA Newsletter - December 2025
- IPTA Newsletter - October 2025
- IPTA Newsletter - June 2025
- IPTA Newsletter - March 2025
- IPTA Newsletter - December 2024
- IPTA Newsletter - October 2024
- IPTA Newsletter - May 2024
- IPTA Newsletter - February 2024
- IPTA Newsletter - November 2023
- IPTA Newsletter - September 2023
- IPTA Newsletter - May 2023
- IPTA Newsletter - March 2023
- IPTA Newsletter - December 2022
- IPTA Newsletter - October 2022
- IPTA Newsletter - July 2022
- IPTA Newsletter - May 2022
- IPTA Newsletter - December 2021
- IPTA Newsletter - October 2021
- IPTA Newsletter - June 2021
- IPTA Newsletter - October 2020
- IPTA Newsletter - June 2020
- IPTA Newsletter - March 2020
- IPTA Newsletter - December 2019
- IPTA Newsletter - September 2019
- IPTA Newsletter - July 2019
- IPTA Newsletter - April 2019
- IPTA Newsletter - December 2018
- IPTA Newsletter - September 2018
- IPTA Newsletter - June 2018
- IPTA Newsletter - March 2018
- IPTA Newsletter - December 2017
- IPTA Newsletter - September 2017
- IPTA Newsletter - December 2016
- IPTA Newsletter - September 2016
Contact
Address
The Transplantation Society
International Headquarters
740 Notre-Dame Ouest
Suite 1245
Montréal, QC, H3C 3X6
Canada
Используйте Вавада казино для игры с бонусом — активируйте промокод и начните выигрывать уже сегодня!